An emergency hypertensive is evidenced by markedly elevated blood
pressure and target organ damage. This situation requires immediate
attention to prevent disability or death. Here, the treatment aim is to
reduce the blood pressure promptly but partially to prevent end-organ
damage without compromising
tissue perfusion. The initial target is to
lower the mean arterial pressure (MAP) by no more than 25%, or reduce the diastolic blood pressure by one-third.
MAP = diastolic blood pressure + [(systolic BP – diastolic BP)/3].
 |
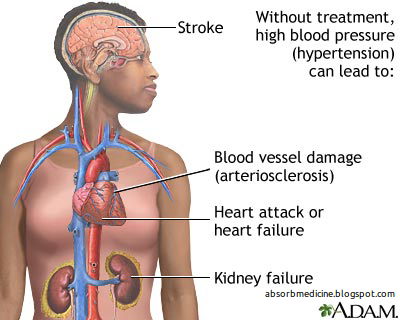
| Mechanisms of Malignant Hypertension. |
Even in the presence of heart failure or hypertensive encephalopathy, a controlled reduction, to a level of about
150/90 mmHg, over a period of 24–36 hours is ideal.
 |
| Hypertensive Urgencies and Treatment. |
 |
| Hypertensive Emergencies and Treatment. |
In most patients, blood pressure can be brought down with
bed rest and
oral medication. Intravenous
labetalol (2 mg/min to a maximum of 200 mg), intravenous
glyceryl trinitrate (0.6–1.2 mg/h), intravenous
sodium nitroprusside (0.3–1.0 mg/kg per min) or
intramuscular
hydralazine (5 or 10 mg repeated at half-hourly intervals) are all effective but require close monitoring.
 |
| Drugs Used in the Treatment of Hypertensive Crises. |
Further reading:
- Kitiyakara C, Guzman NJ. Malignant hypertension and hypertensive emergencies. J Am Soc Nephrol 1998;9:133-42. [PubMed]




I like each of the content material, I have to state we valued, We would love additional information regarding this particular, because of the fact it is very excellent.Thanks concerning exposing.Health Zone
ReplyDelete